Management of anaphylactic shock
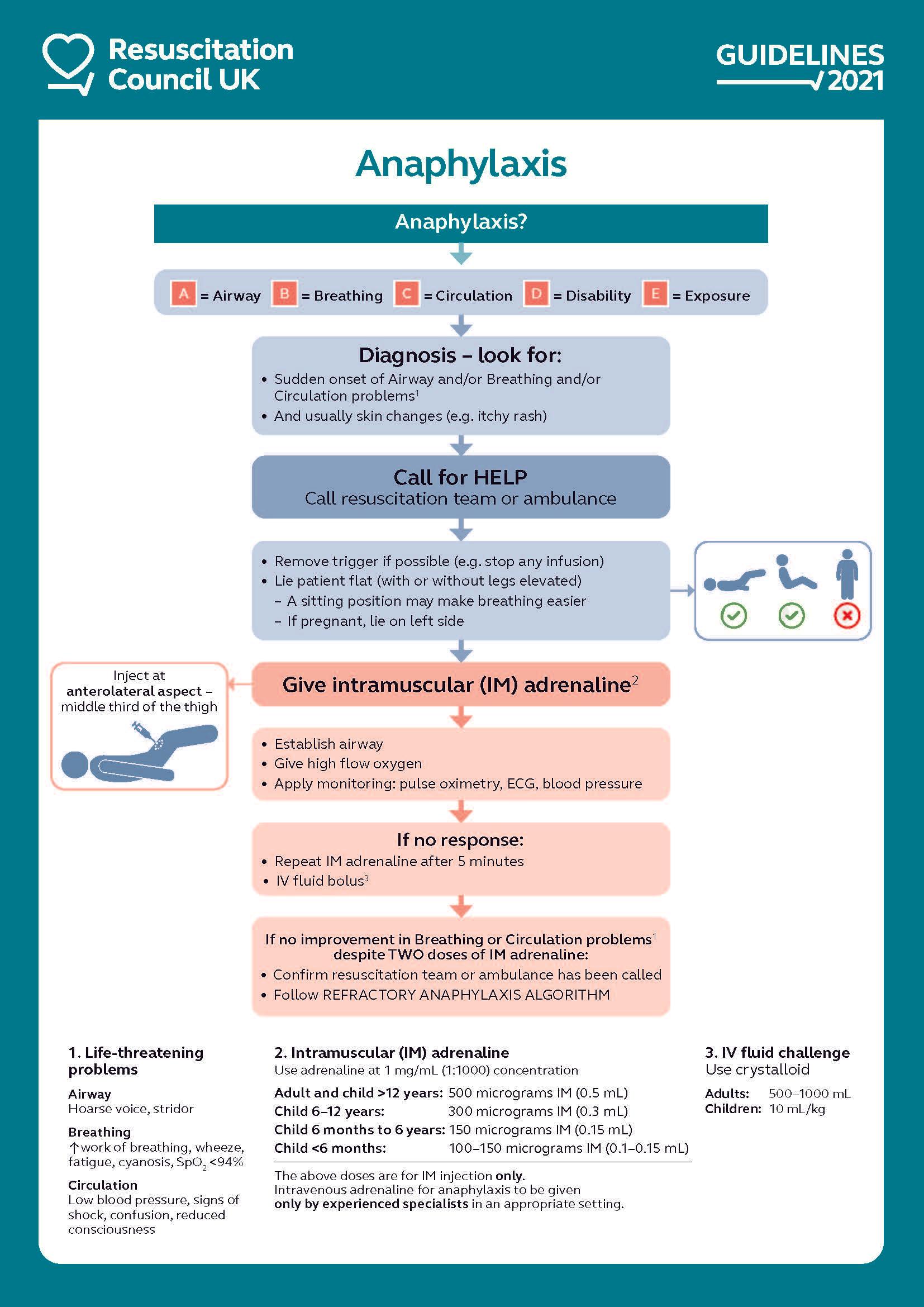
The principles of management are (1):
- to recognize the serious life-threatening condition .
- call for help (don't be proud!)
- assesment of general condition and management based on an ABCDE approach.
- adrenaline therapy if indicated.
- investigation and follow-up by an specialist in allergy
The key steps for the initial treatment of anaphylaxis are shown in the algorithm below.This algorithm is applicable to all healthcare settings (1):
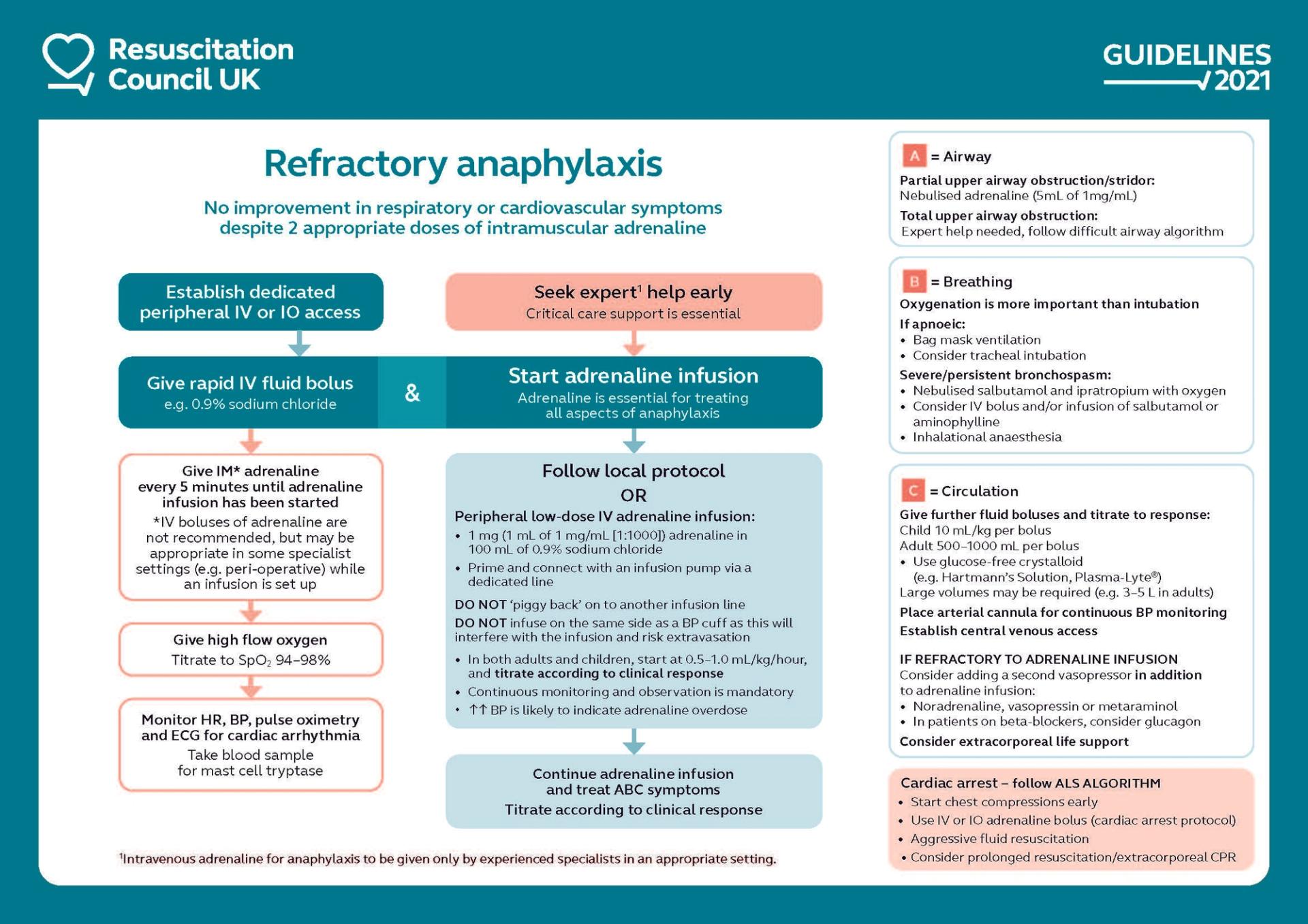
Refractory anaphylaxis is defined as anaphylaxis requiring ongoing treatment (due to persisting respiratory or cardiovascular symptoms) despite two appropriate doses of IM adrenaline (1):
- most of the anaphylaxis reactions occurring in a community setting will respond to initial treatment with IM adrenaline, although currently around 10% receive a second dose and 2.2% (95% confidence interval, 1.1- 4.1%) receive more than two doses
- all healthcare professionals should be able to identify patients with Breathing and/or Circulation problems of anaphylaxis which do not respond to initial treatment with IM re quickly by calling for support from the resuscitation team or from the ambulance service for urgent transfer to hospital
After emergency treatment for anaphylaxis (2):
- adults and young people aged 16 years or older who have had emergency treatment for suspected anaphylaxis should be observed for 6-12 hours from the onset of symptoms, depending on their response to emergency treatment. In people with reactions that are controlled promptly and easily, a shorter observation period may be considered provided that they receive appropriate postreaction care prior to discharge
- children younger than 16 years who have had emergency treatment for suspected anaphylaxis should be admitted to hospital under the care of a paediatric medical team.
Notes:
- antihistamines are not recommended as part of the initial emergency treatment for anaphylaxis (1)
- antihistamines have no role in treating respiratory or cardiovascular symptoms of anaphylaxis
- antihistamines can be used to treat skin symptoms that often occur as part of allergic reactions including anaphylaxis
- their use must not delay treatment of respiratory or cardiovascular symptoms of anaphylaxis (using adrenaline and IV fluids)
- role of antihistamines in anaphylaxis is debated but there is consensus across all guidelines that they are not a first-line treatment
- are of no benefit in treating life-threatening features of anaphylaxis
- antihistamines can be helpful in alleviating cutaneous symptoms (whether these are due to anaphylaxis or non-anaphylaxis allergic reactions), but must not be given in preference to adrenaline to treat anaphylaxis
- in the presence of ongoing Airway/Breathing/ Circulation problems of anaphylaxis, give further IM adrenaline and seek expert advice
- once a patient has been stabilised, use a non-sedating oral antihistamine (e.g. cetirizine) in preference to chlorphenamine which causes sedation
- steroids in anaphylaxis (1)
- routine use of corticosteroids to treat anaphylaxis is not advised
- consider giving steroids after initial resuscitation for refractory reactions or ongoing asthma/shock. Steroids must not be given preferentially to adrenaline.
Reference:
- (1) Emergency treatment of anaphylactic reactions. Guidelines for healthcare providers. Working Group of the Resuscitation Council (UK).2021
- (2) NICE (December 2011). Anaphylaxis: assessment to confirm an anaphylactic episode and the decision to refer after emergency treatment for a suspected anaphylactic episode.
Related pages
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page