Management of UTIs in men
NICE suggest that (1):
- send midstream urine for culture and susceptibility
- immediate antibiotic treatment should be offered
- refer to hospital if a person aged 16 or over has any symptoms or signs suggesting a more serious illness or condition (for example, sepsis)
- if there is a history of fever or back pain, patient should be suspected as having upper UTI and should be managed as possible acute pyelonephritis
- choice of antibiotic 1,2:
- first choice 3
- trimethoprim
- 200 mg twice a day for 7 days
- OR
- nitrofurantoin - if eGFR >=45 ml/minute 4
- 100 mg modified-release twice a day for 7 days
- 100 mg modified-release twice a day for 7 days
- note in previous PHE guidance (2),
- pivmecillinam 400mg STAT then 200mg TDS for 1 week was an alternative first choice antibiotic
- however this has not been advised as an alternative first choice antibiotic for a UTI in a man by NICE
- trimethoprim
- second choice (no improvement in UTI symptoms on first choice taken for at least 48 hours or when first choice not suitable) 3
- 1 see BNF for appropriate use and dosing in specific populations, for example, hepatic impairment and renal impairment.
- 2 doses given are by mouth using immediate-release medicines, unless otherwise stated.
- 3 check any previous urine culture and susceptibility results and antibiotic prescribing and choose antibiotics accordingly.
- 4 nitrofurantoin is not recommended for men with suspected prostate involvement because it is unlikely to reach therapeutic levels in the prostate.
- 5 may be used with caution if eGFR 30-44 ml/minute to treat uncomplicated lower UTI caused by suspected or proven multidrug resistant bacteria and only if potential benefit outweighs risk (BNF, August 2018)
- first choice 3
- reassess at any time if symptoms worsen rapidly or significantly or do not improve in 48 hours of taking antibiotics, sending a urine sample for culture and susceptibility if not already done. Take account of:
- other possible diagnoses
- any symptoms or signs suggesting a more serious illness or condition
- previous antibiotic use, which may have led to resistance
Antibiotics should be avoided in elderly men with asymptomatic bacteriuria (1).
If male under 65 years old then consider (5):
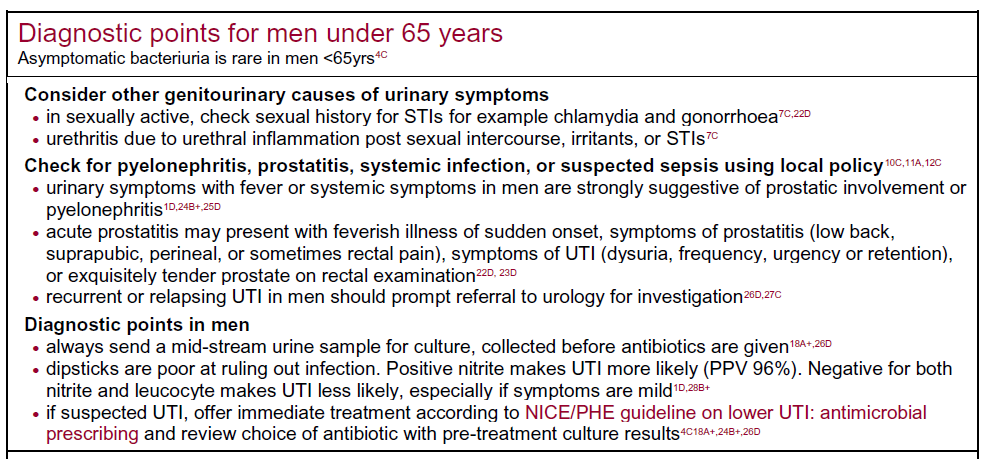
Risk factors for increased resistance include (2):
- care home resident,
- recurrent UTI,
- hospitalisation >7d in the last 6 months,
- non-resolving urinary symptoms,
- recent travel to a country with increased antimicrobial resistance (outside Northern Europe and Australasia) especially health related,
- previous known UTI resistant to trimethoprim, cephalosporins or quinolones
If increased resistance risk, send culture for susceptibility testing & give safety net advice. If GFR<45 ml/min or elderly consider pivmecillinam or fosfomycin (3g stat plus 2nd 3g dose in men 3 days later)
Further investigation/referral depends on various factors (1,2,3,4)
- referral for assessment is not routinely indicated
- however, referral for assessment should be considered for men who have:
- symptoms of upper urinary tract infection (pyelonephritis) (1)
- failure to respond to appropriate antibiotic therapy (1)
- frequent episodes of urinary tract infection (UTI) - this is stated as two or more episodes in a 3-month period or or 3 or more UTIs in the last 12 months
- features of urinary obstruction (e.g. in older men, enlarged prostate)
- history of pyelonephritis, calculi, or previous genitourinary tract surgery
- urgent referral is indicated for men with suspected cancer
- any age with painless macroscopic haematuria:
- if haematuria is associated with symptoms of UTI
- culture the urine before referring
- if UTI is not confirmed by urine culture, or if haematuria does not resolve with treatment of the UTI
- refer urgently
- if haematuria is associated with symptoms of UTI
- recurrent or persistent UTI associated with haematuria, in a male aged 40 years or older
- unexplained microscopic haematuria, in a male aged 50 years or older
- with an abdominal mass identified clinically or on imaging that is thought to arise from the urinary tract
- any age with painless macroscopic haematuria:
- however, referral for assessment should be considered for men who have:
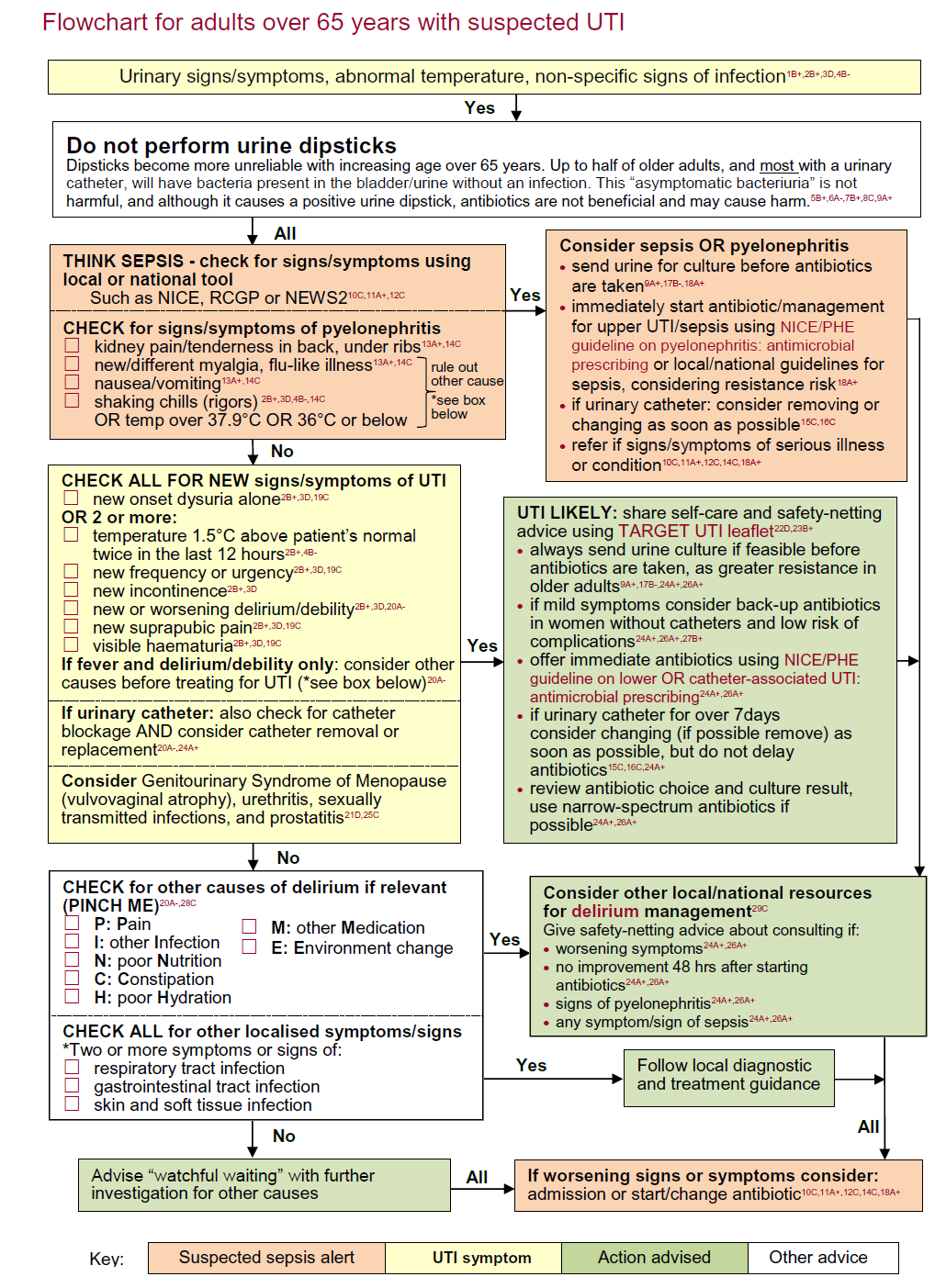
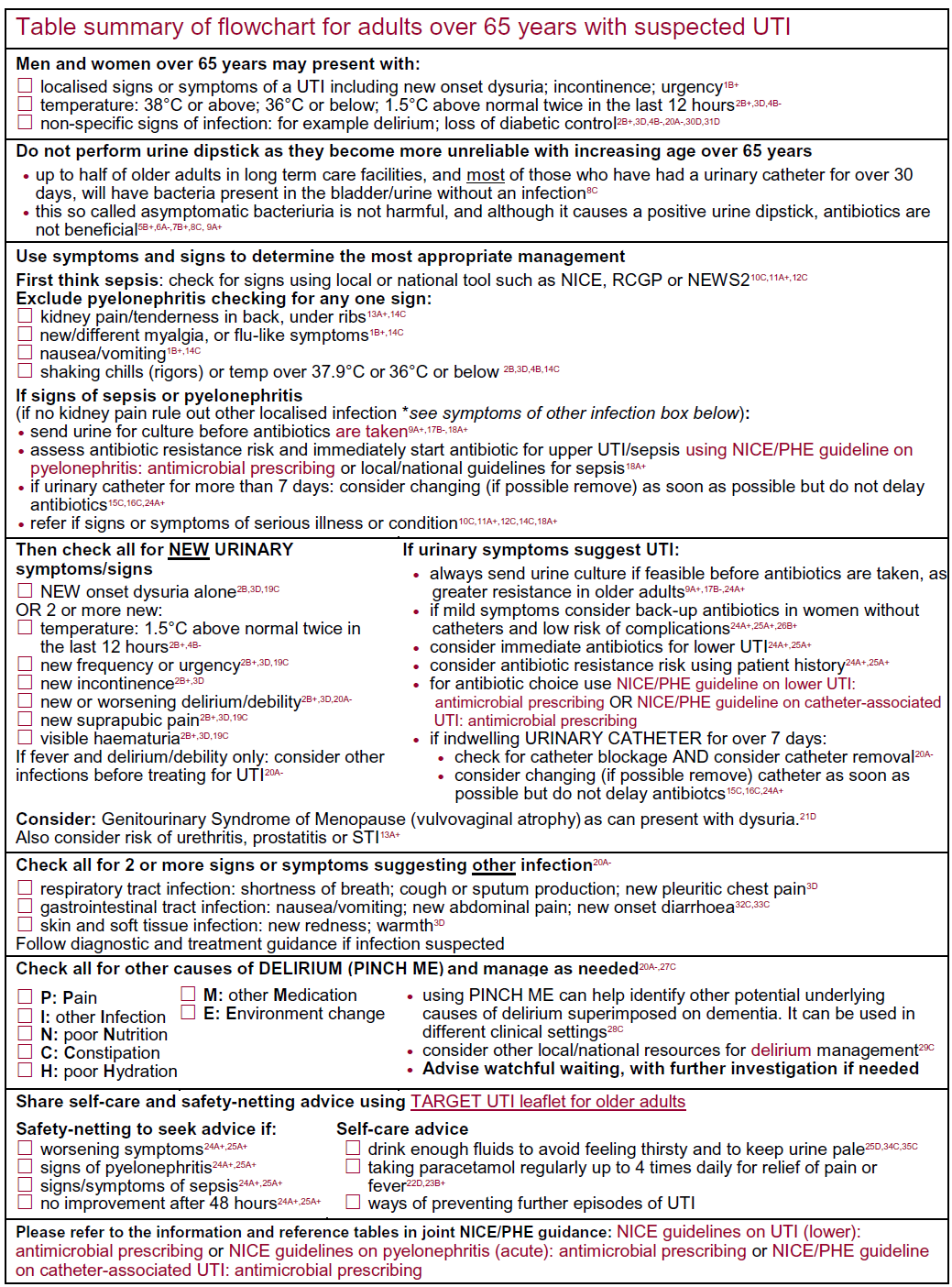
There has been a flowchart developed for the diagnosis and management of ALL adults over 65 years old (5):
Reference:
- NICE (October 2018). Urinary tract infection (lower): antimicrobial prescribing
- Public Health England (October 2014). Management of infection guidance for primary care for consultation and local adaptation
- Harper M, Fowlis G. Management of urinary tract infections in men. Trends in Urology, Gynaecology & Sexual Health 2007;12(1):30-35
- Health Protection Agency (2009). Management of infection guidance for primary care: for consultation and local adaptation
- Public Health England (August 2019). Diagnosis of urinary tract infections - Quick reference tool for primary care for consultation and local adaptation
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page